Healthcare Services: Richie Brace
The Richie Brace® was designed and introduced to the medical community in 1996 by sports podiatrist, Dr. Doug Richie. Since that time the Richie Brace has become a gold standard treatment in the orthotics industry. It is universally recognized by podiatrists, pedorthists, orthotists and orthopedic surgeons as a unique , breakthrough technology to treat a wide variety of foot and ankle pathologies. Many imitations have followed, but none have achieved the fit, comfort and clinical success of the Richie Brace.
Unique Features
Fit and Comfort
The Richie Brace is lighter than most custom ankle-foot orthoses. The leg uprights are designed to leave the front and back of the leg open for breathability and comfort. Once the Richie Brace is positioned on the foot and leg and the Velcro straps are adjusted, the user is hardly aware they are even wearing it.
Easy Application and Removal
After initial adjustment of the three straps, daily application and removal of the Richie Brace involves the simple opening and closing of one single strap. All of the straps of the Richie Brace can be easily and in expensively replaced without the need for rivots or glues.
Download the Richie Brace Order Forms
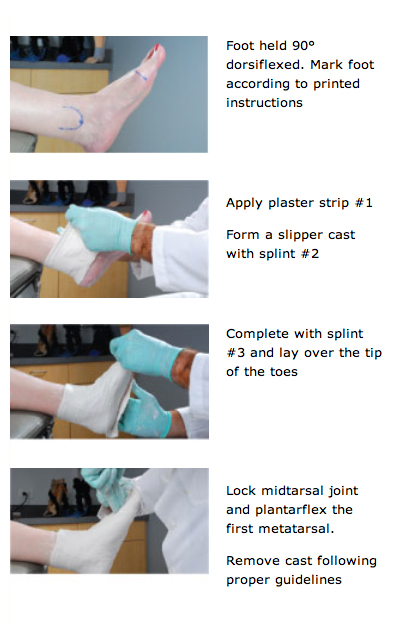
Casting Overview
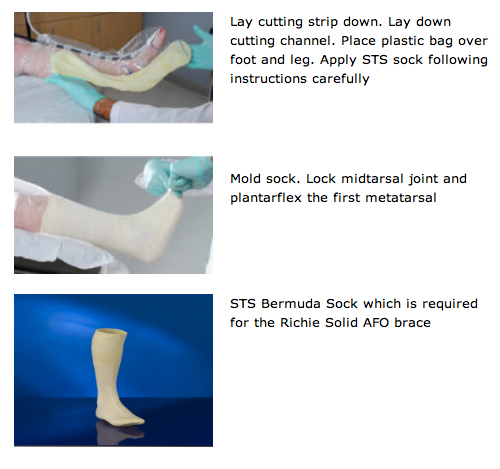
The Richie Brace requires a negative impression cast utilizing either plaster splints or the STS Casting Sock. Neutral suspension technique is recommended while plantarflexing the First Ray. Complete casting instructions are available at www.richiebrace.com. Cast impression required with the STS Mid-Leg Casting Sock from www.stssox.com.
Plaster Casting
STS Sock Casting
Richie Brace Products and Treatment Guide









